INTRODUCTION
This guide has been developed to help you prepare for total hip replacement surgery and provide essential information for post-operative care, recovery, and rehabilitation. While many patients will experience a significant improvement in mobility, function and quality of life, it is important to remember that the original aim of hip replacement surgery was, and still is, to alleviate the pain from arthritis.
HOW DOES THE HIP FUNCTION?
The hip is the major weight-bearing joint connecting the thigh bone (femur) to the pelvis. It is a ball-and-socket type joint, where the top of the thigh bone, called the femoral head, forms the ball and the acetabulum of the pelvis forms the socket. The joint surfaces are lined with a smooth layer of articular cartilage, which cushions the joint and allows for smooth movement.
WHAT IS ARTHRITIS?
As we age, the cartilage in our joints can become damaged and wear down, leading to conditions such as osteoarthritis. This type of arthritis results in the breakdown of the cartilage in the hip joint, causing damage to the joint surface, often resulting in bone-on-bone contact. When Arthritis becomes severe, bone spurs form around the edge of the joint surface and will often be seen on x-rays. Symptoms of arthritis commonly include pain, stiffness, and difficulty walking. Pain may be felt in various areas, including the groin, thigh, buttock, or even the knee and can cause significant disturbance to your sleep at night and to your walking and standing tolerance during the day. Stiffness, sometimes caused by the bone spurs and by inflamed tissues around the joint, can make daily activities, such as putting on shoes or getting out of a car, challenging.
NON-SURGICAL TREATMENTS
For those with hip arthritis, initial treatment often involves non-surgical measures like pain relief medications, anti-inflammatory drugs, and gentle exercise. Weight loss, if applicable, can also help alleviate symptoms. These strategies can significantly improve function and may delay the need for surgical intervention. Even in cases when surgery is indicated, physical activity or formal physical therapy can help ensure your hip will be as strong and mobile as possible which can improve your recovery after surgery. For this reason I always encourage physical therapy for patients with hip arthritis, even if it is “bone-on-bone”.
WHY CONSIDER HIP REPLACEMENT SURGERY?
If conservative treatments fail to manage the pain and stiffness effectively, and your daily activities or sleep are disrupted, a hip replacement might be the best option. This procedure is most suitable when arthritis symptoms severely impact quality of life on a regular basis. Questions I typically ask to help you understand the impact of arthritis:
– Do you limit your activities with loved ones because of your hip pain?
– When it comes to hip pain, do you have more bad days than good days?
– Does your hip impact your ability to maintain your physical health?
– Are you currently using, or considering using, a cane or walker due to hip pain?
If you are answering “yes” to these questions, I think it is at least worth your time to get more information on hip replacement surgery in your unique situation.
TIMING YOUR SURGERY
While hip replacement is effective, it is a major surgery and has a small but significant risk of complication. Hip replacement surgery should only be considered after trying other options, such as weight loss, physical therapy, and medication. Surgery is typically recommended when arthritis symptoms make daily life unmanageable. Waiting too long does not necessarily worsen outcomes; the right time for surgery is when pain and limitations significantly affect your life. Hip replacement surgery is a choice, and you should not feel pressured into subjecting yourself to surgery.
SUCCESS RATE OF HIP REPLACEMENTS
Hip replacement surgery is one of the most successful orthopedic procedures. Over 90% of patients report high satisfaction, and many resume normal activities within six months, often forgetting they ever had an issue. While there are many success videos with patients very active immediately after surgery, there are also many patients that take longer to heal. Give yourself time to heal after surgery and do not compare yourself to others, Typical recovery is 6-12 weeks.
THE SURGERY
Total Hip Replacement (THR) involves replacing the damaged ball and socket with artificial components made of metal, plastic, or ceramic. The procedure can be performed using various approaches, including the anterior technique, which involves minimal muscle disruption and may lead to quicker recovery. The operation is done under spinal or general anesthesia, and recovery protocols involve early mobilization. Formal physical therapy after hip replacement is not always necessary.
PREPARATION FOR SURGERY
Before your operation, you will undergo a thorough health assessment to ensure your safety. This may include seeing a specialist physician and attending a pre-admission clinic. Engaging in pre-operative exercises can improve strength and flexibility, aiding in recovery. Additionally, preparing your home for a safe recovery environment is essential. Ensure you have reviewed your medications with your team, some medicines need to be stopped 1 week before surgery, such as weight loss drugs (Ozempic or similar medications), and blood thinners (Aspirin / Plavix)
HOSPITAL STAY AND AFTERCARE
After surgery, a large majority of patients will be discharged home on the same day. Cases that are performed late in the afternoon will sometimes require an overnight stay in hospital. A patient may spend a few days in the hospital after a revision or complex cases requiring additional surgery. Rarely, a first time (primary) total hip replacement will also be admitted after surgery if special circumstances exist, such as situations that make discharge home unsafe. Please discuss this with the team if you believe this is necessary as it requires special permission from most insurance companies.
RETURNING TO NORMAL ACTIVITIES
Recovery timelines vary based on individual circumstances. While light activities can often resume within weeks, more demanding tasks or sports may require several months. Always consult your surgeon before resuming any strenuous activities.
General expectations for recovery (individual cases vary):
– Return to driving between 2-4 weeks, once off narcotics and requiring a cane or less for walking
– Return to sedentary work (desk based duties) 6 weeks
– Return to manual labor 12 weeks
RISKS AND LONGEVITY OF HIP REPLACEMENTS
Hip replacements are highly durable, often lasting decades. The following chart from a New Zealand Registry Study, demonstrates your risk of needing a revision surgery for your hip replacement based on your age when the first hip replacement is performed:
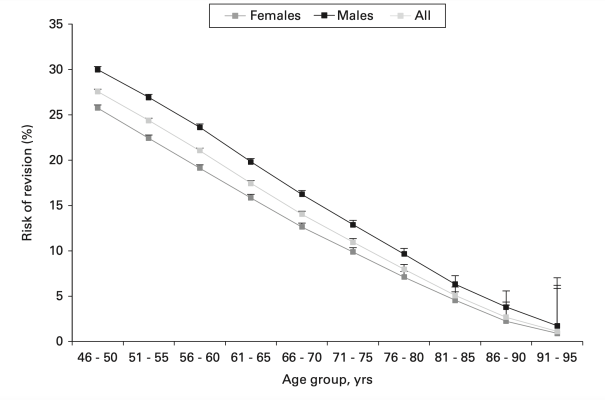
As you can see, even patients in their 40’s still have a 70% + chance of never requiring another hip replacement surgery for the rest of their lives. However, there are still significant risks associated with the surgery, such as infection, blood clots, or nerve injury, though these are rare. Proper pre- and post-operative care can help minimize these risks.
Please review the following risks of surgery:
RISKS
As with all procedures, total hip replacement carries some risks and potential complications.
UNCOMMON: (1-3%)
- Blood clots: A DVT (deep vein thrombosis) is a blood clot that can form in a vein, often presenting as red, swollen, and painful legs. The risk of DVT increases after surgery, especially orthopedic procedures. While DVTs are treatable and typically not dangerous, they can travel to the lungs and cause a pulmonary embolism (PE), which is a serious condition that affects breathing. You will be on a blood thinner after surgery for 1 month to prevent this and we also recommend wearing compression stockings for the first week. Early mobilization and walking is the best ways to reduce the risk of blood clots.
- Bleeding: Bleeding during surgery is usually minimal and controlled. Rarely, excessive bleeding may occur. In rare cases, bleeding may cause a hematoma (a large bruise or blood clot) near the wound and rarely may result in increased drainage. Please notify our team if you experience these issues.
- Pain: Postoperative pain in the hip is expected. If the pain is significant, inform your medical team so that appropriate pain management can be provided. Pain should improve over time, but in rare cases, it may persist. This may be due to soft tissue irritation, stretching of muscles, tendons and ligaments that have be shortened for a prolonged time, nerve irritation around the hip, other complications, or no clear cause.
- Altered wound healing: The wound may become red, thickened, or painful (keloid scarring), especially in individuals with darker skin tones. Scar massage with cream after healing may help.
LESS COMMON: (1-2%)
- Infection: Antibiotics will be administered before and after surgery, and the procedure will be performed in sterile conditions. Despite these measures, infections occur in about 1-2% of cases. Signs include redness, warmth, pain, or fluid discharge from the wound. Mild infections of the incision may be treated with antibiotics, while more severe infections or infections that involve the implants require surgical cleaning and sometimes removal of the implant. In rare instances, the infection can lead to sepsis (a serious blood infection).
- Prosthesis wear/loosening: Modern surgical techniques and implants ensure that most hip replacements last over 15 years. However, in some cases, the implant may wear out or loosen earlier due to unknown reasons, overuse, or infection. Revision surgery may be required to replace the implant if this occurs
- Altered leg length: After surgery, the operated leg may appear slightly longer or shorter than the other leg. It is common to have a sensation of leg lengthening as arthritis has worn out the joint surface and causes shortening over a long time. Correcting the leg to the proper length usually involves restoring about 5mm (1/4″) to the leg and this sudden change is quickly detected by your body. Persistence of this sensation is uncommon and you should give your body time to adjust. Avoid using corrective devices for at least 12 months after surgery.
- Joint dislocation: The hip joint may dislocate after surgery. In most cases, the joint can be realigned without additional surgery. However, if dislocations recur or cannot be resolved non-surgically, revision surgery or a brace may be necessary.
- Nerve damage: Nerves near the hip may be injured during surgery, resulting in temporary or permanent changes in sensation or weakness. The sciatic nerve is particularly at risk in posterior hip replacements and the femoral nerve is at risk in anterior hip replacements.
RARE: (<1%)
- Bone damage: The thigh bone or pelvis bone may fracture when the implant is inserted. If this occurs, it may require additional fixation during or after surgery.
- Blood vessel damage: Rarely, blood vessels may be damaged, requiring additional surgical repair by a vascular surgeon.
- Pulmonary embolism: A PE, caused by a blood clot traveling to the lungs, can make breathing difficult and may be life-threatening.
- Death: While extremely rare, death can occur as a result of one or more of the above complications or due to complications from anesthesia.
**For a comprehensive guide to total joint replacement, including information on preparation and daily recovery expectations, please see Dr Andrew Wickline’s total hip or knee replacement guides found here:
Knee Booklet
For 10% off – Use discount code: SPENCER10
Dr. Andrew Wickline’s Total Hip Replacement Guide